In endodontic practice, performing treatments through crowns or bridges represents a true clinical challenge. Lack of visibility, limited access, and anatomical complexity demand a technical and precise approach.
In this article, we present a real case performed by Dr. Noé Hernández, in which an endodontic treatment was carried out on tooth 27 through a four-unit fixed bridge, achieving a predictable and conservative outcome.
Diagnosis
The patient attended Dr. Hernández’s practice complaining of pain in the second quadrant.
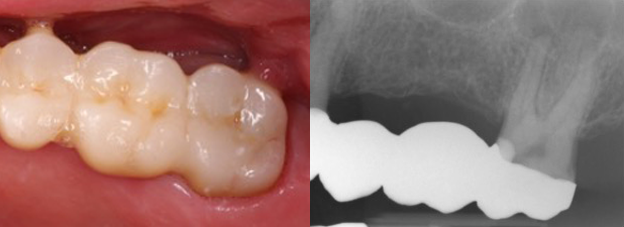
Clinical examination revealed a long bridge covering several teeth, including tooth 27. This tooth presented a deep cervical restoration, very close to the pulp horn, which raised suspicion of endodontic involvement.
The diagnostic tests performed included:
- Negative vitality test
- Positive percussion test
- Physiological probing
The diagnosis was pulp necrosis with chronic apical periodontitis.
Facing the treatment: necropulpectomy through the bridge
One of the main challenges in this case was performing access through the bridge without compromising its structure, due largely to the lack of light and visibility inside the pulp chamber.
For this purpose, a high-speed diamond bur was used to remove the porcelain without fracturing it, followed by a transmetal bur to create access through the metallic part of the bridge.
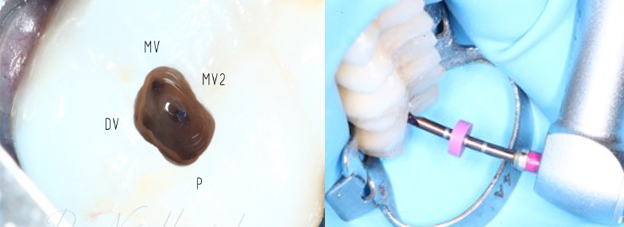
Once inside, four canals were located, and the following endodontic sequence was carried out:
- Coronal preflaring using the BlueShaper PRO® Z1 file at 500 rpm up to two-thirds of the working length
- Glide path with #10 hand files
- Complete instrumentation using the basic sequence of the BlueShaper PRO® system by Zarc: Z1, Z2, Z3, and Z4
In necrotic cases like this, proper irrigation is essential to eliminate necrotic tissue and bacterial load.
In this case, the following irrigation protocol was used:
- 4.25% sodium hypochlorite, ultrasonically activated with Z-Activator in three 30-second cycles.
- 17% EDTA, also activated for 30 seconds to ensure final cleaning of the dentinal tubules.
Obturation was performed using the thermocompaction technique with Z-Condensor, ensuring a three-dimensional seal of the canals.
The final radiographic result showed complete instrumentation and obturation of the four canals, respecting the internal anatomy of the tooth and preserving the integrity of the prosthetic bridge.
